






About Us
Executive Editor:Publishing house "Academy of Natural History"
Editorial Board:
Asgarov S. (Azerbaijan), Alakbarov M. (Azerbaijan), Aliev Z. (Azerbaijan), Babayev N. (Uzbekistan), Chiladze G. (Georgia), Datskovsky I. (Israel), Garbuz I. (Moldova), Gleizer S. (Germany), Ershina A. (Kazakhstan), Kobzev D. (Switzerland), Kohl O. (Germany), Ktshanyan M. (Armenia), Lande D. (Ukraine), Ledvanov M. (Russia), Makats V. (Ukraine), Miletic L. (Serbia), Moskovkin V. (Ukraine), Murzagaliyeva A. (Kazakhstan), Novikov A. (Ukraine), Rahimov R. (Uzbekistan), Romanchuk A. (Ukraine), Shamshiev B. (Kyrgyzstan), Usheva M. (Bulgaria), Vasileva M. (Bulgar).



 PDF
PDFThe new key specialty, General Practitioner (GP), was introduced to render general health care at the primary care level. Further intensification of health reforms, radical improvements to healthcare structures and the quality of medical care are currently in progress. Special consideration is being given to the improvement of (i) SVP activity, (ii) quality of the diagnosis and treatment of disease, and disease prevention policy.
Hypertension is the most commonly encountered condition that requires constant medical supervision by the GP in the course of the disease. Hypertension currently ca be regarded as a pandemic causing social and economical losses to society [1]. The worldwide prevalence of hypertension is sufficiently high and comes to 18-20 %; this figure increases with age and reaches 62 % in those aged 60 years and older. [2]. A number of researches relevant to the diagnoses and treatment of this state were conducted. However, doctors still find it difficult to prevent the development of various complications resulting in treatment failures [3]. Primary health care physicians in Uzbekistan often pay more attention to patients who present to polyclinics, while the main risk group for complications includes patients who have high levels of blood pressure but are not aware of it or not undergoing regular treatment for hypertension [4, 5, 6]. Early diagnosis of hypertension, the reduction of the effect of risk factors and supervised treatment of high blood pressure are the main tasks of outpatient health care providers.
This survey was aimed at evaluating general practitioners activity regarding their approach to the management of hypertensive patients, including their knowledge, skills, scope and quality of rendered services.
Materials and methods
With a view to study general practitioners activity 90 physicians of regional SVPs were selected. Information was collected by the teachers of the postgraduate training centers for GP professional development. SVP physicians were interviewed according to a special questionnaire that covered such data as: work experience, type of retraining within the program of training for general medical practice, participation in short-term cycles of continuous professional education. Aspects of physician activity such as work load, problems in supervising hypertensive patients; prescription of medical examination, non-drug treatment and drug therapy were evaluated. In addition to the questionnaire, the physicians knowledge and skills was assessed by testing and their skills were evaluated by direct observation of their consultation of patients with "hypertension" diagnosis in a mock clinical situation; medical records on hypertensive patients made by each particular physician were studied as well.
Outcomes and discussion
1. Analysis of questionnaire findings
Based on the questionnaire findings the total medical experience of GPs was more than 4 years, out of these 48 % of physicians worked in SVP over 4 years, 40 % of physicians for 2-3 years. Because young doctors and graduates of medical universities are unwilling to work in rural SVPs, there were only 12 % of them. 58 % of SVP physicians, having only basic medical education as therapists or pediatricians, were retrained under a national 10 months program for general practitioners. 34 % of physicians underwent a 3-month retraining as GPs, 18 % of physicians were not GP trained. 75 % of the SVP physicians had participated in the specialized short-term cycles within the framework of the continuous medical education system 71 % of GP were certified for a category (level of physicians´ knowledge and skills like GP) in 2004-2007: 17 % of GPs were of higher category, 50 % of first and 33 % of second category. The analysis of SVP physicians´ workload showed that on average one GP receives 20-25 patients daily. Most of the GPs asserted that the number of patient visits had been considerably increasing over recent years which entailed considerable increased load on SVP and its staff. 36% of physicians noted that the number of visits to SVP had doubled. The study suggested that this growth in patients´ visits to SVP was caused by (i) concomitant reduction of visits to the central district hospital or to the policlinic (according to 96 % physicians); (ii) people had started to pay more attention to their health (according to 69 % physicians) and therefore sought advice whereas previously they may not have done so.
To assess the SVP general practitioners´ knowledge and skills in their approach to managing hypertensive patients, the GPs were asked if they found it difficult to diagnose and treat hypertensive patients. 8 % of physicians stated that they had difficulties managing 18-49 years old hypertensive patients; and 26 % of physicians said the medical supervision of 50-60 years old patients was complicated for them.
Following the answers 72 % of physicians by themselves made ECG of hypertensive patients during last month, 69 % of physicians conducted regular medical check up and full examination of hypertensive patients according to the standard (National Clinical Guideline on diagnostics, treatment and prevention of hypertension in adults at primary health care). 46 % of physicians recommended promotion of healthy life style in order to reduce risk factors.
2. Evaluation of physicians´ skills by observation of medical examination of hypertensive patients
In order to further assess how physicians work, their skills were directly observed when the physicians were examining hypertensive patients in SVP. 83 % of physicians measured ABP (arterial blood pressure) correctly under the standard. Their consultation skills were assessed on the following: whether information was given to patients regarding his/her status, whether the results of the clinical examination was given and medication. Following the observation results: 75 % of physicians informed patients about their health state and examination results, 94 % of physicians recommended next visit and made appointments, 84 % of physicians referred patients to have various laboratory tests, 57 % of physicians explained the results, 23 % of physicians identified body-weight index. Thus not all physicians consult hypertensive patients in line with the established procedure. Experts noted that GPs insufficiently inform patients about hypertension risk factors, effects on target organs, side effects of drugs and consequences of not following the prescribed therapeutic regimen.
3. Evaluation of general practitioners knowledge about diagnostic methods and treatment of hypertensive patients
Knowledge was assessed according to tests developed by GPs Trainers. The test contained several optional answers for each question, but three of them were considered as the most appropriate ones due to their specific applicability to SVP settings (see picture 1).
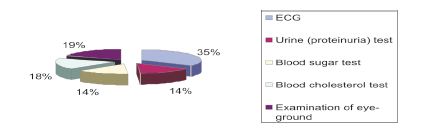
Picture 1. Investigations in patients with Hypertension
All physicians marked necessity of ECG analysis, but only 42 % of them considered detection of proteinuria as a reasonable procedure, and 41 % of physicians considered detection of blood sugar as an impractical test though the above three tests are regarded as able to be performed in SVP settings. Blood cholesterol test is mainly done in the central rayon
hospital and not all SVP physicians possess an ophthalmoscope or are able to use one to examine the fundus.
In the following test the physicians were asked to select out of the following six situations which three patients merited measuring the ABP by the GP, see picture 2.
In Uzbekistan, the General practitioner measures ABP in all pregnant women and in patients with clinical symptoms as well as in patients who were invited to SVP for prеvented medical examination. In other cases ABP is measured by the districts (patronage) nurse. The test findings showed that 86 % of physicians measure ABP of pregnant women, 64 %
- of patients with clinical symptoms of hypertension and only 31 % of them invited of patients to SVP for examination. To ensure efficient teamwork, prior to the patient seeing the GP the SVP nurse measures the ABP of all patients presenting to the SVP regardless of the purpose of their visit. The nurse fills in an outpatient medical record and writes down main findings including the ABP. Where the ABP is 140/90 mm Hg or higher, she marks it with red color and notifies the physician about the patient´s high level of ABP. The physician must then recheck the ABP measurement twice on one arm, and if the ABP level is high, measure it on the other arm. Unfortunately, the tests results show that this rule is not followed by all SVP physicians.
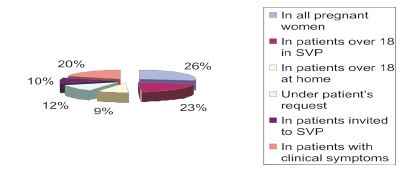
Picture 2. ABP measuring by GP
In SVPs physicians must examine hypertensive patients following national clinical guidelines, i.e. they should carry out and read ECG, test the urine for protein, and carry out a blood sugar test and examination of the optic fundus. However, we found that only 26 % of physicians carried out a full examination of clinic patients, incorporating these four examination components. Hence not all physicians follow recommendations of the clinical guidelines and carry out a comprehensive medical examination in SVP settings.
4. Evaluation of hypertensive patients´ medical records
GP Trainers evaluated the thoroughness of completion of medical records of hypertensive patients by the following criteria:
- Records of screening for early signs of hypertension and ABP measurements;
- Presence of ECG, urine and blood sugar tests, description of examination of the fundi;
- Carrying out a risk profile for the diagnosis of cardiovascular disease and adding into the diagnosis information regarding the ABP level and level of risk;
- Records of recommendations fornon-drug treatment and specific medications.
Summary of the evaluation of patient medical records is shown in Picture 3.
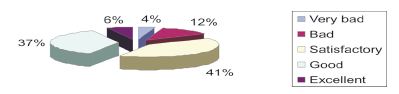
Picture 3. Evaluation of hypertensive patient medical records
Based on the analysis of patient medical records: 92 % of these had recorded the ABP, 53 % showed that diagnosis was correctly made after two measurements within 2 months; in 61% a diagnosis of «arterial hypertension» was recorded correctly with indication of the degree and risk. Blood sugar tests had been recorded in 30 % of hypertensive patients medical records as part of regular medical checkups, as were urine (proteinuria) test (in 59 %) and examination of fundi (16 %). Entry of an ECG were found in 71 % of patient medical records, and body-weight index in 13 % ones. Risk profiling in the diagnosis of cardiovascular disease was not shown in all hypertensive patients´ medical records. Thus, smoking status was indicated only in 20 % of patient medical records, a history of cardiovascular disease in 32 %, and degree of risk assessed in 24 %. Recommendations on reduction of risk factors, and non-drug treatment were entered in 31 % of patient medical records. Prescription of diuretics, as a first-line medication, with consideration of indications and contraindications, was shown in 28 % of patient medical records. Follow up observation of patients took place every 3-6 months with corresponding notes in 61 % of patient medical records. In 49 % of patient medical records there were notes regarding treatment effectiveness resulting in a decrease in blood pressure after 3-6 months on prescribed treatment.
Probably, of patient medical records management could be ascribed to work overload or carelessness in completing the patient medical records. In the approach to the management of hypertensive patients it will be necessary to draw physicians´ attention particularly to the issues of follow up observation, ABP control and efficiency of prescribed treatment.
So, application of various techniques in the study enabled us to identify discrepancies in the results. Thus, in the questionnaires physicians correctly answered most of the questions related to diagnostics and treatment of hypertensive patients. However, in consultations they insufficiently informed patients about their disease, the suitability of treatment undertaken, or the side effects of medicines. Finally, the analysis of patient medical records shows that even being aware of clinical guidelines recommendations, physicians do not record their consultations adequately or fully. They give little attention to true confirmation of diagnosis and to recommendations of drug-free treatment.
Therefore it is reasonable to train physicians in hypertension management within the framework of continuous medical education, to provide them with national clinical guidelines on hypertension, and regularly conduct monitoring of physicians work by the instrumentality of the GP training centers teachers.
References
- Chobanian A. Et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. - JAMA, 2003, May 21; 2560-71. European Society of Cardiology guidelines for the management of arterial hypertension, Guidelines Committee. J. Hypertens. - 2003. - V.21, №6. - P. 1011-1053.
- European guidelines on cardiovascular disease prevention in clinical practice. Guy De Backer, Ettore Ambrosioni, Knut Borch-Johnsen et all // European Heart Journal. - 2003. - №24. - P. 1601-1610.
- Карпов Ю.А. Клиническая гипертензиология: анализ завершенных исследований 2001-2002 гг. // Кардиология. - 2002. - №10. - С. 62-66.
- Мамедов М.Н., Оганов Р.Г. Артериальнаягипертониявклинической практике врача: современная стратегия диагностики и лечения // Медицина. -2005. - №3. - С. 10-16.
- Оганов Р.Г., Галкин В.А., Масленникова Г.Я. Артериальная гипертония - проблема поликлиническая // Тер.архив. - 2006. - №1. - С. 6-9.
- Ощепкова Е.В., Довгалевский П.Я., Гриднев В.И. Регистр артериальной гипертонии // Тер. архив. -2007. - №1. - С. 48-52.
Narmukhamedova N.A. EVALUATION OF GENERAL PRACTITIONERS’ ACTIVITY IN RURAL HEALTHCARE CENTRES OF UZBEKISTAN. International Journal Of Applied And Fundamental Research. – 2011. – № 1 –
URL: www.science-sd.com/387-23459 (23.07.2026).