






About Us
Executive Editor:Publishing house "Academy of Natural History"
Editorial Board:
Asgarov S. (Azerbaijan), Alakbarov M. (Azerbaijan), Aliev Z. (Azerbaijan), Babayev N. (Uzbekistan), Chiladze G. (Georgia), Datskovsky I. (Israel), Garbuz I. (Moldova), Gleizer S. (Germany), Ershina A. (Kazakhstan), Kobzev D. (Switzerland), Kohl O. (Germany), Ktshanyan M. (Armenia), Lande D. (Ukraine), Ledvanov M. (Russia), Makats V. (Ukraine), Miletic L. (Serbia), Moskovkin V. (Ukraine), Murzagaliyeva A. (Kazakhstan), Novikov A. (Ukraine), Rahimov R. (Uzbekistan), Romanchuk A. (Ukraine), Shamshiev B. (Kyrgyzstan), Usheva M. (Bulgaria), Vasileva M. (Bulgar).



Medical sciences
 PDF
PDF1 Introduction
According to Russian official statistics, on average hundreds of thousands of new cases of tuberculosis and lung cancer are diagnosed every year. Computed tomography is the first and obligatory procedure for such patients. Over the past decade the development of endoscopic technologies contributed to the widespread implementation of thoracoscopic lungs surgery, in particular with the purpose of morphological verification of various processes in the trachea, bronchi and lung tissue. Besides, it should be taken into consideration that thoracoscopia is undoubtedly related to minimally invasive surgical interventions although they are less advantageous than, say, transbronchial lungs biopsy. However, when choosing the method, a crucial role belongs to the tumor localization, the patient’s individual characteristics and medical personnel qualifications [1].
2 Material and methods
These surgeries are of high complexity and require highly trained surgeons [2]. To assist in the preparation for the thoracoscopic surgery they have developed a software solution which can be used in thoracic surgery at the stage of the diagnostic evaluation of lungs affection. The program is implemented in MeVisLab [3], which is a platform for medical data post-processing obtained by means of X-ray diagnostics in order to develop applications prototypes using in clinical settings.
The proposed software solution operates with raw data of DICOM format that have earlier been obtained during the compulsory examination of the patient on the CT scan. Basic data package is downloaded into a program for constructing a three-dimensional reconstruction of the thoracic cage that provides integral perception of the internal lung and thoracic cage macrostructure of the patient as a whole [4].
To build the most accurate model of the lungs, it is a good idea to provide a high quality of image resections. Then, due to the natural difference in optical density, the skeletal system, lungs, the bronchial tree and the tumor itself are visualized very well. It will help us to build an elaborated three-dimensional reconstruction of the probable object of the research and to carry out the necessary manipulations with it, for instance, to turn on / off the pleura and/or ribs and the vertebral column, to identify the diaphragm position, to compare the positions of the patient during the surgery [5]. The program allows you to calculate the volume and the distance of any elements of the model as well as to automatically simulate the so-called “lung collapse” during the first piercing and not only in the terms of the volume but also the shape that makes possible to predict the inevitable displacement of the tumor.
Further, the surgeon may consider various options of thoracoports arrangement and choose the best (“comfortable”) variant of the surgery in regard to the selected pathological object.
Besides the angle of surgery action, the program has also implemented additional surgical approaches criteria [6], which are the area of availability, soft tissues thickness that are traversed by manipulators to the possible point of surgical intervention and the length of the manipulator in the pleural cavity. The visual perception of mutual spatial arrangement of the pathological process and its interrelation with surrounding structures allow us, in accordance with the peculiarities of the focus of a disease, to make the choice of the best possible strategy of surgical intervention.
Simulation of the surgical process and/or anatomical structures makes it possible to differentiate features and details that give an opportunity to the surgeon to make and to check a pre-surgical concept not only with regard to the nature of pathological changes but also to the choice of the strategy of the surgery, the scope of the work and to the predictions of the most likely risks of the coming surgery.
Thus, the work of the surgeon dealing with the program consists in the following:
At the first stage they choose the research area, which will be used for building. DICOM raw data are downloaded into the program for constructing a three-dimensional reconstruction of the area of interest. The program allows you to choose the color scale, which makes it possible to highlight the necessary structure (Fig.1).

Figure 1 – 3D model of the lungs with highlighting the basic elements
The second stage of a virtual surgery involves an “intraoperative revision” that is a visual check of the area of interest from different perspectives. Virtually we have access to all areas, to which the access is obstructed during surgical intervention, by changing the transparency of the tissue and turning off the elements of the model (Fig. 2a), as well as an arbitrary secant line (Fig.2b). Of course, the doctor will not be able to palpate the body organ but he or she can examine it in details. Then, the user of the program should express his or her own desire to see the possible “lung collapse” (Fig.3).
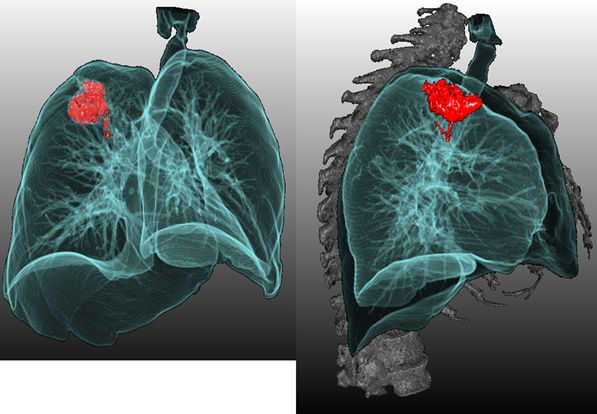
Figure 2 - 3D-model of the lungs а) without ribs and the vertebral column
b) a lateral secant line passing through the tumor
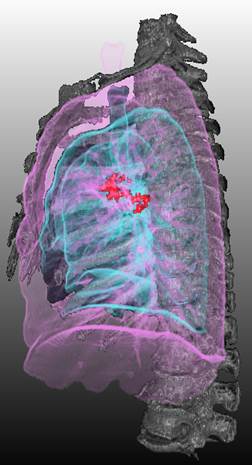
Figure 3- 3D-model of the left lung (the original one is pink and the “collapsed” one is blue)
At the third stage a doctor needs only to “take and to place manipulators” so that they would coincide with the tumors but would not pass through the bone tissue of the patient and would be located as more convenient as possible for the coming surgery. The program shows the angles between thoracoports (Fig.4) and the submerged depth of each of them (Fig.5).
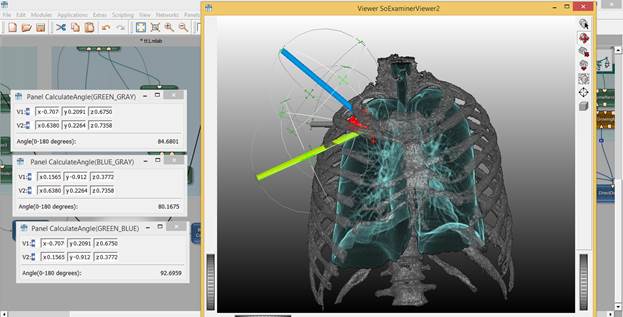
Figure 4. The example of thoracoports arrangement (coronal view) and the angles between them
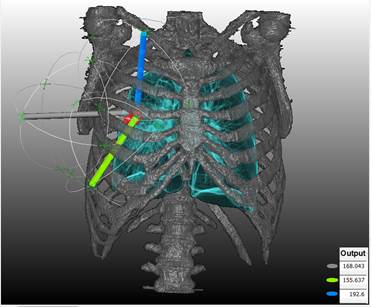
Figure 5 The example of thoracoports arrangement indicating the submerged depth of each of them
By simulating the process of surgery, the specialist is able to produce a variety of manipulations concerning the obtained image on the monitor, for instance, to rotate it in different planes, zoom it and zoom out, make resections, include additional elements of the model.
3 Results
In mode of semi-transparent surfaces a 3D-reconstruction gives a comprehensive picture of the area of interest, allows us to see the internal structure of the body organ and/or tumor invasion into adjacent organs. The surgeon, having radiological data and a simulation program of the surgery process, virtually takes the necessary actions using obtained images on a computer monitor. The model makes it possible to notice the individual state of the lung, bronchial tubes and blood vessels branching even on the basis of non-contrast researches.
4 Conclusions and Discussions
This software solution helps to make up a plan dedicated to possible surgery intervention for a particular patient. The doctor chooses the strategy about a coming surgery based on the entire data complex: 2D resections of DICOM-package and his or her personal experience on the one hand and additional prompts of a three-dimensional simulation system on the other hand.
A developed system of 3D-visualization in thoracic surgery increases self-descriptiveness of a standard radial patient examination which allows us to see in detail a possible surgical intervention and/or it can be widely used to improve the skills of medical personnel.
2. Video endoscopic interventions on the organs of the abdomen and retroperitoneum: a Guide for physicians. Edited by. A.E. Borisova. Saint-Petersburg: Enterprise EFA, Janus 2002
3. MeVisLab [Electronic resource] Medical image processing and visualization. - Mode of access: http://www.mevislab.de/ 23.12.2012
4. Markina S.S., Tsymbaliuk N.N. System of 3d simulation of thorascopic operations in view of tumorous lesions of lungs. Mezdunarodnyj naucno-issledovatel'skij zurnal. 2013, 4 (11): 124-125
5. Garvey C, Hanlon R. Computed tomography in clinical practice. BMJ 2002; 324:1077
6. Bondarev A.A., Myasnikov A.D., Rabotsky I.A. Criteria for assessing surgical approaches in endosurgery. 2003; 4: 47-53
Medvedev D.., Markina S.. 3D PRE-SURGICAL SIMULATION OF THORACOSCOPIC LUNG SUGERY. International Journal Of Applied And Fundamental Research. – 2016. – № 5 –
URL: www.science-sd.com/467-25060 (23.07.2026).